Panic disorder refers to a chronic anxiety condition marked by recurrent, unexpected panic attacks alongside persistent fear of future episodes. It works by triggering the body’s fight-or-flight response without any real threat, producing overwhelming physical and emotional reactions.
The main symptoms of panic disorder include rapid heartbeat, shortness of breath, chest pain, dizziness, and intense fear. Common causes range from genetic predisposition and neurological imbalances to chronic stress and trauma.
The primary treatments include psychotherapy, particularly cognitive behavioural therapy, medication such as SSRIs, diazepam, and structured lifestyle changes. Diazepam works by enhancing GABA activity in the brain to quickly calm an overactive nervous system during acute episodes. In the UK, diazepam is a prescription-only controlled substance, typically accessed through an NHS GP or a regulated online pharmacy.
What is Panic Disorder?
Panic disorder is a diagnosable anxiety disorder under the DSM-5 classification, characterised by recurring, unexpected panic attacks and persistent anxiety about their recurrence. According to the review article published in Dialogues in Clinical Neuroscience (2015) by the Department of Psychiatry and Psychotherapy at the University Medical Centre Göttingen, large-scale epidemiological surveys conducted under the auspices of the National Institute of Mental Health (NIMH) and other international research consortia found that up to 33.7% of the population experience an anxiety disorder, including panic disorder, at some point in their lifetime.
According to Professor Ahmed Hankir, MBChB, MRCPsych, honorary visiting professor at the School of Medicine, Cardiff University, and lead psychiatrist at Private Therapy Clinic, “Panic disorder is a mental health condition where you have, one, recurring panic attacks, and two, you develop a persistent fear of having more. This fear can change your behaviour. Avoiding places where a panic attack might happen, not going out alone, and constantly worrying about your health. It’s not just the attacks, it’s the anxiety between them that becomes disabling.”

The condition was formally recognised in the late 20th century after decades of evolving psychiatric classification. The difference between normal anxiety and a panic attack is that normal anxiety is a proportionate response to a genuine stressor, whereas a panic attack involves a sudden surge of intense fear with severe physical symptoms, often arising without an apparent trigger and driven by the body’s fight-or-flight response.
What is the History of Panic Disorder?
The history of panic disorder dates back to ancient times, when the condition was broadly described under the umbrella of “melancholia” by Greek physicians attempting to explain episodes of overwhelming fear without a clear cause.
In the 19th century, soldiers returning from battle reported clusters of symptoms, including a racing heart, breathlessness, and chest tightness, documented under the term “irritable heart,” or what later became known as war neurosis. Sigmund Freud in 1895 described a distinct condition he termed “anxiety neurosis,” characterised by episodes of acute psychological and physical distress tied to accumulated tension.
Panic disorder was officially classified as a distinct condition in the DSM-III in 1980, separating it from broader anxiety states and establishing the clear diagnostic criteria that remain the foundation of clinical practice today.
What is The Difference Between a Panic Attack and Panic Disorder?
The difference between a panic attack and panic disorder is that a panic attack is a single, acute event, whilst panic disorder is a persistent, long-term condition. A panic attack is a sudden and intense episode of fear with physical symptoms like a racing heart, choking sensation, or shortness of breath that typically peaks within 10 minutes and resolves on its own.
Panic disorder, by contrast, is a long-term condition characterised by recurrent unexpected panic attacks along with symptoms of ongoing fear of future attacks and behaviour changes designed to avoid triggers, such as refusing to use public transport or avoiding crowded spaces.
What are The Symptoms of Panic Disorder?
The symptoms of panic disorder include emotional, physical, and behavioural disruptions that can significantly affect everyday functioning and quality of life.
The symptoms of panic disorder are listed below.
- Emotional Symptoms: Emotional symptoms of panic disorder include fear of losing control, fear of dying, and intense distress caused by rapid heartbeat, chest pain, breathlessness, dizziness, and sweating.
Emotional symptoms of panic disorder are listed below.
- Rapid heartbeat: Rapid heartbeat symptoms are the sensation of the heart pounding or racing uncontrollably, often mistaken for a cardiac event, and include palpitations, rhythm irregularity, awareness, and an overwhelming sense of imminent physical danger.
- Sweating: Sweating symptoms refer to sudden, excessive perspiration without physical exertion that includes cold sweats, clammy skin, and heightened self-consciousness in social or public settings.
- Shortness of breath: Shortness of breath symptoms refer to the sensation of being unable to breathe adequately, including tight breathing, hyperventilation, and a choking sensation that can escalate feelings of panic rapidly.
- Chest pain: Chest pain symptoms refer to sharp, pressing, or squeezing discomfort in the chest that frequently causes individuals to fear they are experiencing a heart attack during a panic episode, making it one of the most distressing symptoms.
- Dizziness: Dizziness symptoms are light-headedness, unsteadiness, or a spinning sensation that causes individuals to feel as though they may faint or lose physical control of their bodies.
- Fear of losing control: Fear of losing control symptoms refer to a powerful belief that one may act erratically or cause a scene, which drives the mental health cycle of avoidance, shame, and anticipatory anxiety.
- Fear of dying: Fear of dying symptoms are the intense, irrational conviction during a panic attack that death is imminent, sustained by the severity of physical symptoms such as chest pain and breathlessness.
- Physical Symptoms
Physical symptoms of panic disorder include hyperventilation, tingling or numbness, hot flushes or chills, chest pain, dizziness, sweating, shortness of breath, and rapid heartbeat.
Physical symptoms of panic disorder are listed below.
- Hyperventilation: Hyperventilation refers to rapid, shallow breathing during an attack, which reduces carbon dioxide levels in the blood, triggering further dizziness and tingling sensations in the extremities that worsen the episode.
- Tingling or numbness: Numbness or tingling in the hands, feet, or around the mouth occurs as a direct result of altered blood flow and hyperventilation, and is a hallmark physical sign during an acute attack.
- Hot flushes or chills: Sudden waves of heat or cold that wash over the body contribute to the physical sense of instability and helplessness that defines a panic attack.
- Behavioural Symptoms
Behavioural symptoms of panic disorder include avoidance behaviour, safety-seeking behaviour, and social withdrawal as attempts to prevent or manage future panic episodes.
Behavioural symptoms of panic disorder are listed below.
- Avoidance behaviour: Deliberately steering clear of places, situations, or activities associated with previous panic attacks, which can progressively restrict a person’s social and occupational functioning.
- Safety-seeking behaviour: Relying on specific objects, people, or routines, such as always sitting near an exit, to manage anxiety, an approach that reinforces rather than reduces fear over time.
- Social withdrawal: Pulling away from relationships and social commitments due to the embarrassment of having a public attack or the exhaustion of constant vigilance.
Is Panic Disorder a Mental Illness?
Yes, panic disorder is a mental illness, specifically classified as an anxiety disorder characterised by recurrent, unexpected panic attacks and persistent fear of future episodes. The condition is formally recognised in the DSM-5 as a distinct diagnosable disorder with clear clinical criteria.
The main causes of panic disorder include neurological dysregulation, genetic predisposition, and environmental stress. Despite its severity, panic disorder is often treatable with therapy and medication, and many individuals achieve full functional recovery with appropriate professional support.
What are The Causes of Panic Disorder?
The causes of panic disorder include a combination of psychological, biological, and lifestyle factors that interact to heighten vulnerability to recurrent panic attacks.
The causes of panic disorder are listed below.
- Psychological Causes: Psychological causes of panic disorder mean the mental and emotional factors arising from thought patterns, past traumatic experiences, and fearful interpretations of bodily sensations that condition the brain to remain in a state of heightened alert and amplify normal physical feelings into perceived emergencies.
Psychological causes include trauma and adverse life events (the lasting neurological impact of distressing experiences like abuse or bereavement), cognitive distortions (habitual catastrophic thinking that assumes worst-case outcomes), and anxiety sensitivity (fearing anxiety symptoms themselves, such as interpreting a slightly elevated heartbeat as a sign of serious illness).
- Biological Causes: Biological causes of panic disorder refer to innate physiological and neurochemical factors rooted in genetic inheritance, neurotransmitter balance, and the brain functioning of fear-processing structures that directly influence the body’s automatic stress responses without any conscious trigger.
Biological causes include genetic predisposition (inherited susceptibility, making first-degree relatives up to eight times more likely to develop panic disorder), neurotransmitter imbalances (dysregulation of serotonin, norepinephrine, and GABA affecting mood and fear), and amygdala dysregulation (heightened reactivity in the brain’s fear centre, causing neutral stimuli to trigger fight-or-flight responses).
- Lifestyle Causes: Lifestyle causes of panic disorder mean the daily habits, environmental pressures, and substance use patterns that gradually deplete the nervous system’s adaptive capacity and lower the threshold for panic attacks.
Lifestyle causes include chronic stress (prolonged exposure to high-pressure work, relationships, or finances), stimulant use (excessive caffeine, nicotine, or recreational stimulants that elevate physiological arousal), and poor sleep hygiene (insufficient or disrupted sleep that impairs emotional regulation and increases stress sensitivity).
What are The Common Triggers of Panic Attacks?
The common triggers of panic attacks are listed below.
- Stressful life events: Major transitions, such as bereavement, redundancy, or relationship breakdown, frequently precipitate a first episode and a quick diagnosis.
- Physical illness: Conditions including hyperthyroidism or cardiac arrhythmias can mimic or directly trigger panic symptoms, reinforcing the pattern of fear.
- Caffeine and stimulants: High doses of caffeine, energy drinks, or recreational drugs rapidly trigger attacks in susceptible individuals by spiking central nervous system arousal.
- Crowded or enclosed spaces: Environmental settings associated with previous attacks become conditioned triggers through learned avoidance.
- Certain medications: Some prescription drugs, including corticosteroids and certain decongestants, can elevate physiological arousal and precipitate episodes.
- Sleep deprivation: Insufficient sleep lowers the neurological threshold for panic, increasing the likelihood of attacks in otherwise ordinary situations.
How Panic Disorders Are Diagnosed?
The main ways to diagnose panic disorder are listed below.
- Clinical interview: A clinician conducts a structured interview to gather a detailed history of symptoms, their frequency, their onset, and their functional impact on daily life.
- DSM-5 criteria: Diagnosis is confirmed when a patient meets the DSM-5 criteria, including recurrent unexpected panic attacks and at least one month of persistent concern about further attacks or significant behavioural change.
- Medical examination: Physical assessments, including blood tests and ECGs, rule out underlying conditions, such as thyroid disorders or cardiac arrhythmias, that are not life-threatening but can mimic panic symptoms.
- Psychological questionnaires: Validated tools such as the Planic Disorder Severity Scale (PDSS) quantify symptom severity and are used to track treatment progress.
- Differential diagnosis: Clinicians must confirm symptoms are not better explained by another disorder, such as PTSD or generalised anxiety disorder, before reaching a final panic disorder diagnosis.
Are Panic Attacks Fatal?
No, panic attacks are not fatal, though their symptoms can feel acutely life-threatening in the moment. Symptoms such as a racing heart, chest pain, and shortness of breath closely resemble those of a heart attack, which is why individuals frequently present to A&E during or after an episode.
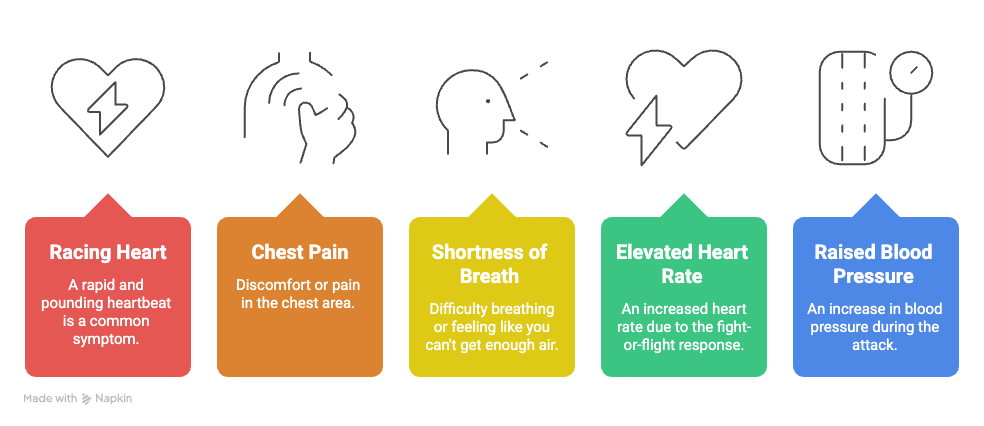
However, panic attacks are intense but temporary surges of fear that usually peak within 10 minutes and resolve naturally without causing lasting physical harm. The physiological changes driven by the fight-or-flight response, such as elevated heart rate and raised blood pressure, are transient and manageable. Understanding that a panic attack is not life-threatening is itself a clinically significant step, as it can directly reduce the severity of anticipatory anxiety and break the cycle of fear.
What To Do During a Panic Attack?
The things to do during a panic attack include controlled breathing, grounding techniques, self-affirmation, staying present, seeking support, and muscle relaxation to reduce panic and restore calm.
Tips to stop a panic attack are listed below.
- Practise controlled breathing: Slow diaphragmatic breathing, inhaling for four counts, holding for four, exhaling for four, counteracts hyperventilation and signals to the nervous system that no genuine threat is present.
- Use grounding techniques: The 5-4-3-2-1 method, identifying five things you can see, four you can touch, three you can hear, two you can smell, and one you can taste, anchors awareness in the present moment and interrupts catastrophic thinking. Regular use of this hack can support the long-term cure of panic attack patterns by reducing fear responses.
- Affirm it will pass: Internally reminding yourself “This will pass in a few minutes; I am not in danger” directly challenges the cognitive distortions sustaining the episode.
- Avoid fleeing the situation: Where safe to do so, remaining in the triggering environment, rather than escaping it, is central to managing panic attack cycles long-term, as avoidance reinforces the learned association between the setting and danger.
- Seek support: Contacting a trusted person or, if symptoms are severe and prolonged, NHS 111, provides reassurance and interrupts the isolation that amplifies panic.
- Apply progressive muscle relaxation: Systematically tensing and releasing muscle groups reduces physical tension and supports the body’s natural recovery from the stress state.
Can Panic Disorder Be Cured?
No, panic disorder cannot be cured as there is no fixed and permanent cure, but it is one of the most highly treatable mental health conditions available to clinicians today. Most individuals can achieve long-term remission and manage symptoms effectively with the right combination of intervention and self-management.
Common treatment approaches, such as psychotherapy and medication, are aimed at reducing symptoms to a manageable level, improving day-to-day functioning, and restoring a full quality of life. A doctor plays a central role in designing and overseeing the treatment plan, as the best outcomes consistently arise from a combination of evidence-based therapy and, where clinically appropriate, carefully supervised pharmacological support.
What are The Treatment Options for Panic Disorder?
The treatment options of panic disorder involve a structured, multi-modal approach addressing the psychological, pharmacological, and lifestyle dimensions of the condition. The treatments of panic disorder are listed below.
- Psychotherapy: Psychotherapy is a structured talk treatment where a doctor or therapist helps a person change panic-related thoughts, feelings, and behaviours. It works by identifying fear patterns, correcting catastrophic thinking, and reducing avoidance behaviours that maintain panic disorder.
Cognitive Behavioural Therapy (CBT) is the most common and effective psychotherapy. It also includes Exposure Therapy, MBCT, cognitive restructuring, interoceptive exposure therapy, breathing retraining, relaxation techniques, psychoeducation, and regular sessions with a doctor or licensed therapist. The benefits include reducing the frequency and intensity of panic attacks, lowering fear of future attacks, improving confidence in managing symptoms, preventing relapse, and improving daily functioning and quality of life.
According to the research paper “Absolute and relative outcomes of psychotherapies for eight mental disorders: a systematic review and meta‐analysis,” published in World Psychiatry, the absolute response rate for psychotherapy in patients with panic disorder was 0.38 (95% CI: 0.33–0.43), meaning 38% achieved at least a 50% symptom reduction.
- Medication: Medication is the use of prescribed medicines to reduce panic symptoms by regulating brain chemicals linked to fear, anxiety, and stress responses. Panic disorder meds work by balancing neurotransmitters such as serotonin and norepinephrine, which helps reduce panic attacks, anxiety sensitivity, and physical symptoms like rapid heartbeat or dizziness.
It includes Selective Serotonin Reuptake Inhibitors (SSRIs), Serotonin-Norepinephrine Reuptake Inhibitors (SNRIs), benzodiazepines for short-term use, and regular monitoring, dose adjustment, and follow-up care by a doctor. The benefits include reducing sudden panic attacks, controlling severe physical symptoms, improving sleep and concentration, helping during intense symptoms, and supporting psychotherapy effectiveness.
According to a 2022 BMJ network meta-analysis (PROSPERO CRD42020180638), SSRIs achieve a 66.4% SUCRA ranking for remission in panic disorder with low adverse events.
- Improving Lifestyle and Self-Management: Lifestyle and self-management are daily habits and coping strategies that help reduce stress, improve body regulation, and prevent panic symptoms from worsening. This approach works by lowering physical stress triggers, improving nervous system stability, and helping people respond calmly instead of fearfully during anxiety sensations.
It includes regular exercise, healthy sleep routines, limiting caffeine, balanced nutrition, mindfulness, relaxation practice, journaling symptoms and triggers, and following treatment plans from the doctor. The benefits include reducing anxiety sensitivity, improving emotional control, supporting better sleep and energy, lowering relapse risk, and strengthening long-term recovery and independence.
Is Seeing a Doctor Necessary Before Taking Panic Disorder Medications?
Yes, seeing a doctor is necessary before taking panic disorder medications because self-prescribing carries significant clinical risks, including inappropriate dosing, dangerous drug interactions, and masking of underlying medical conditions that require alternative treatment.
Medical supervision is required to ensure medications are prescribed at the correct therapeutic dose and that the patient’s response is monitored over time. Before prescribing, a doctor evaluates and monitors several critical factors: reviewing full medical history, identifying comorbid conditions such as depression or substance use disorder, ruling out underlying physical conditions, such as thyroid disorders or cardiac arrhythmias, that may present with similar symptoms, and carefully assessing the suitability of specific medications in light of individual risk factors, including the risk of dependence with benzodiazepines.
What Are the Best Medications for Panic Disorder?
The best medications for Panic Disorder include several pharmacological options spanning different mechanisms of action and clinical profiles. The medications for Panic Disorder are listed below.
- Sertraline (SSRI): Sertraline is the most widely prescribed first-line medication for panic disorder in the UK, stabilising serotonin levels to reduce both attack frequency and background anxiety, with effects typically emerging over four to six weeks.
- Escitalopram (SSRI): Escitalopram is a highly selective SSRI with a robust evidence base for panic disorder and a well-tolerated side-effect profile, often preferred for individuals with sensitivity to adverse effects.
- Venlafaxine (SNRI): Venlafaxine is an effective alternative to SSRIs that targets both serotonin and norepinephrine pathways, providing broader symptom coverage, particularly where comorbid depression is present.
- Clonazepam (Benzodiazepine): Clonazepam is a longer-acting benzodiazepine used for short-term management of acute panic symptoms, prescribed with caution due to the potential for physical dependence.
- Diazepam (Benzodiazepine): Diazepam is a fast-acting benzodiazepine that rapidly reduces acute panic symptoms by calming the central nervous system, typically prescribed for short-term relief only under close medical supervision in the UK.
- Imipramine (TCA): Imipramine is a tricyclic antidepressant with demonstrated efficacy in panic disorder, generally reserved for patients who have not responded adequately to first-line options.
- Propranolol (Beta-blocker): Propranolol is a beta-blocker that addresses physical symptoms of panic, including rapid heartbeat and trembling, rather than the underlying anxiety, often used as a short-term adjunct in situational panic management.
How Does Diazepam Help Manage Panic Disorder Symptoms?
Diazepam helps manage panic disorder symptoms by acting as a fast-acting sedative that enhances the neurotransmitter GABA to calm an overactive nervous system, dampening the rate at which nerve signals fire and suppressing the body’s exaggerated fear response.
Once ingested, diazepam binds to GABA-A receptors in the brain, potentiating the inhibitory effect of GABA and producing a rapid reduction in anxiety, muscle tension, and psychological agitation. Diazepam reduces symptoms such as racing thoughts, chest pain, and trembling within 15 to 60 minutes, providing meaningful, measurable relief during acute episodes. However, diazepam is typically used for short-term relief rather than long-term treatment due to the clinically established risk of tolerance.
What to Know About Safely Obtaining Diazepam in the UK for Panic Disorder?
Things to know about safely obtaining diazepam in the UK for panic disorder are listed below.
- Prescription requirement: Diazepam is a prescription-only medicine in the UK; patients must consult a GP or licensed prescriber to obtain it legally and safely.
- NHS and private routes: Diazepam may be prescribed via an NHS GP for qualifying patients or through regulated private online clinics operating under Care Quality Commission (CQC) oversight.
- Controlled drug regulations: As a Schedule 4, Class C controlled drug, diazepam prescriptions are subject to strict dispensing regulations — prescriptions are typically issued for short durations only to minimise dependence risk.
- Regulated online pharmacies: Patients may access diazepam through GMC-registered online pharmacies verifiable via the MHRA register, following a digital consultation with a licensed UK doctor.
- Avoiding unregistered sources: Purchasing diazepam from unregistered online sellers carries serious legal and health risks, including counterfeit products and potential criminal liability under the Misuse of Drugs Act 1971.
- Monitoring and clinical review: Safe use requires regular follow-up with a prescriber, who is obligated under UK clinical guidelines to assess for tolerance and dependence, adjusting or discontinuing the prescription as clinically appropriate.
Can Patients Buy Diazepam for Panic Disorder Without a Doctor’s Prescription in the UK?

No, patients cannot buy diazepam for panic disorder without a doctor’s prescription in the UK because diazepam is a legally controlled substance, and its supply without a valid prescription constitutes a criminal offence under the Misuse of Drugs Act 1971. In terms of its legal classification, diazepam is a Class C, Schedule 4 controlled drug under UK law, meaning its manufacture, distribution, and possession are subject to strict Home Office regulation.
However, in emergencies or for special cases, some online shops like ours help people buy diazepam in UK. Though this is rare, it is tightly restricted and always governed by clinical and legal accountability. Individuals should be aware that attempting to obtain diazepam via unregistered channels exposes them to serious legal, health, and safety risks.
To manage panic disorder effectively, it helps first to recognise common panic disorder symptoms, such as palpitations, sweating, and a fear of losing control. Understanding the causes of panic disorder, including genetic, psychological, and environmental factors, is also important.
Instead of relying on unprescribed meds, patients should consider evidence-based treatments like cognitive behavioural therapy (CBT). When medication is needed, doctors may prescribe appropriate medications for panic disorder and panic attacks, such as SSRIs or SNRIs, which are safer and less addictive than some other panic attack meds out there.
