Vertigo is now a common issue of the inner ear or neurology in the UK and other countries. Affecting around 21.6% people globally, it works by sending faulty signals between the inner ear and brain. This triggers disorientation without any actual motion occurring.
Vertigo presents in two primary types, such as peripheral vertigo and central vertigo, each with distinct origins. Common symptoms of vertigo include a spinning sensation, balance problems, nausea, and abnormal eye movements. It is typically caused by conditions such as BPPV, Ménière’s disease, vestibular neuritis, head injury, migraine, or neurological conditions. Treatment for vertigo ranges from vestibular rehabilitation exercises and natural remedies to prescription medications.
When it comes to medication for vertigo, diazepam is used for acute vertigo, which suppresses central nervous system activity to reduce spinning sensations. In the UK, diazepam is a controlled drug and requires a valid prescription, though in certain emergency circumstances, some registered pharmacies may facilitate access under supervised clinical conditions.
What is Vertigo?
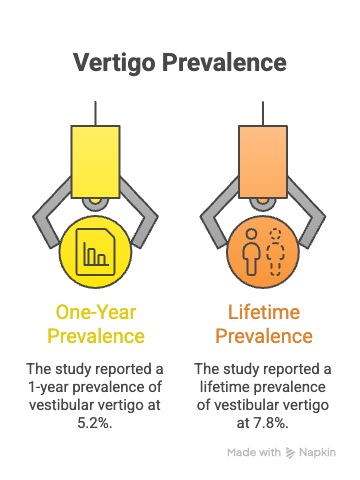
Vertigo is a neurological symptom characterised by a false sense of rotational or linear movement, arising from dysfunction in the vestibular system of the inner ear or brain pathways. According to research by H. K. Neuhauser, MD, MPH, M. von Brevern, MD, A. Radtke, MD, F. Lezius, M. Feldmann, T. Ziese, MD, and T. Lempert, MD, PhD, published in the Neurology Journal in 2005, a widely cited epidemiological study reported a 1-year prevalence of vestibular vertigo at 5.2% and a lifetime prevalence of 7.8%.
According to Dr Sepehr Oliaei, a board-certified otolaryngologist specialising in ear, nose and throat disorders, “The most common uh vertigo that people refer to is benign positional vertigo. That usually happens when tiny microscopic crystals come loose inside the inner ear organ of balance. They’re usually attached to these hairlike fibres inside the inner ear. Those crystals move through the canals of the inner ear. They wreak havoc, and they cause dizziness.”
Vertigo was first formally described in medical literature in the 19th century, when clinicians began distinguishing it from general dizziness using early DSM-aligned diagnostic frameworks. The difference between vertigo and dizziness is that dizziness refers to a general sense of lightheadedness or unsteadiness, whereas vertigo specifically involves a spinning or rotational illusion caused by balance problems rooted in the inner ear or central nervous system.
What is the History of Vertigo?
The history of vertigo traces back to ancient civilisations, where spinning sensations were linked to spiritual possession or humoral imbalance. The term derives from the Latin vertere, meaning ‘to turn,’ and was referenced in 16th-century medical texts to describe disorienting physical states involving involuntary movement perception.
By the 19th century, clinicians began separating vertigo as a distinct medical condition from broader forms of dizziness, identifying it as a symptom tied to the inner ear and neurological dysfunction. The discovery of the semicircular canals’ role in balance further shaped understanding of different types of vertigo, including what we now classify as peripheral and central vertigo.
The 20th century brought refined diagnostic criteria and the identification of specific conditions, such as BPPV and Ménière’s disease, that produce vertigo’s hallmark spinning sensations, cementing its place as a formally categorised medical symptom.
What are The Types of Vertigo?
The types of vertigo include peripheral vertigo and central vertigo.
The types of vertigo are listed below.
- Peripheral Vertigo: Peripheral vertigo is a vestibular disorder originating in the inner ear or the vestibular nerve, typically causing intense spinning, nausea, and hearing disturbances. It feels like a sudden, severe room-spinning episode often triggered by head position changes, and may include different symptoms such as tinnitus and pressure in the ear.
- Central Vertigo: Central vertigo is a neurological condition caused by dysfunction in the brainstem or cerebellum, producing persistent imbalance and a less-intense but longer-lasting spinning sensation. It feels like continuous unsteadiness rather than sudden spinning, and may accompany different symptoms such as double vision, slurred speech, and difficulty walking.
What are The Symptoms of Vertigo?
The symptoms of vertigo include spinning sensations, balance problems, nausea and vomiting, abnormal eye movements, and hearing-related disturbances, each reflecting the vestibular system’s failure to process spatial orientation accurately.
The symptoms of vertigo are listed below.
- Spinning Sensation: Spinning sensation refers to a false perception of rotational movement, either of the person or their surroundings, caused by abnormal vestibular signalling in the inner ear or brain. It includes episodes of intense dizziness, disorientation, and an inability to focus visually; emotionally, it commonly triggers irritability, frustration, and anger due to the unpredictable and distressing nature of attacks.
- Balance Problems: Balance problems are disruptions in postural stability arising from impaired coordination between the vestibular system, eyes, and proprioceptive nerves. They include difficulty walking in a straight line, stumbling, and frequent falls; physically, they may manifest as pacing, restlessness, hand movements, shaking, and unsteady legs as the body attempts to compensate for faulty spatial signals.
- Nausea and Vomiting: Nausea and vomiting are autonomic responses triggered by conflicting sensory input between the vestibular system and visual cortex, mimicking the brain’s reaction to ingested toxins. These symptoms include persistent queasiness, retching, and vomiting, and often worsen with any head movement or visual stimulation during an active vertigo episode.
- Eye Movement (Nystagmus): Nystagmus refers to involuntary, repetitive oscillatory eye movements caused by abnormal activation of the vestibulo-ocular reflex during a vertigo episode. It includes rhythmic horizontal, vertical, or rotational eye movements that impair vision and may provide clinicians with diagnostic clues regarding the type and location of vestibular dysfunction.
- Hearing-Related Symptoms: Hearing-related symptoms are auditory disturbances, including tinnitus, muffled hearing, and a sensation of ear fullness, that accompany vertigo when the inner ear is affected. They include low-frequency hearing loss and intermittent sound sensitivity, particularly associated with Ménière’s disease, where fluctuating endolymphatic pressure disrupts both balance and auditory function simultaneously.
Understanding the duration of vertigo can be really helpful for figuring out the cause behind it.
How Long Does Vertigo Last?
Vertigo lasts between a few seconds and several days, depending on the underlying vertigo causes and the specific vestibular structures involved. BPPV episodes are typically the briefest, lasting seconds to under a minute, as they are triggered by displaced calcium crystals shifting with head movement.
Ménière’s disease episodes tend to last between 20 minutes and several hours, driven by fluctuating endolymphatic fluid pressure. Vestibular neuritis causes the most prolonged episodes, with acute spinning sensations lasting days and residual balance disruption persisting for weeks as the inflamed vestibular nerve recovers.
What are The Causes of Vertigo?
The causes of vertigo include BPPV, Ménière’s disease, vestibular neuritis, head injury, migraine, and neurological conditions, each disrupting the vestibular system through distinct pathophysiological mechanisms.
The causes of vertigo are listed below.
- BPPV (Benign Paroxysmal Positional Vertigo): BPPV is a mechanical inner ear disorder caused by displaced calcium carbonate crystals (otoliths) that migrate into the semicircular canals, generating false motion signals. It is the most common cause of vertigo and is uniquely triggered by specific head position changes, such as rolling over in bed or tilting the head upwards.
- Ménière’s Disease: Ménière’s disease is a chronic inner ear condition caused by the abnormal accumulation of endolymphatic fluid, leading to episodes of vertigo, tinnitus, and progressive hearing loss. It is unique in that it produces a triad of symptoms, such as vertigo, ear pressure, and fluctuating hearing loss, and its episodes are unpredictable in frequency and duration.
- Vestibular Neuritis: Vestibular neuritis is an inflammatory condition of the vestibular nerve, most commonly caused by a viral infection, resulting in sudden, severe vertigo without hearing loss. Its unique feature is an abrupt onset that resolves over days, though central compensation may take weeks, leaving residual unsteadiness.
- Head Injury: Head injury is a traumatic event that disrupts vestibular structures, including the semicircular canals, otolith organs, or central pathways, resulting in post-traumatic vertigo. When it comes to head injury, vertigo may manifest immediately or emerge weeks after the injury, particularly following a concussion or temporal bone fractures.
- Migraine: Migraine is a neurological disorder that, in its vestibular variant, produces recurrent vertigo episodes with or without headache due to abnormal cortical spreading and brainstem dysfunction. For this, vertigo may be the primary symptom, preceding or occurring independently of the characteristic migraine headache.
- Neurological Conditions: Neurological conditions, including multiple sclerosis, stroke, and cerebellar atrophy, cause central vertigo by disrupting vestibular processing in the brainstem or cerebellum. These conditions produce persistent, variable vertigo that does not respond to standard vestibular repositioning manoeuvres and requires specialist neurological diagnosis.
How is Vertigo Diagnosed?
The main ways to diagnose vertigo are listed below.
- Clinical History Review: A clinician evaluates onset, duration, triggers, and associated symptoms to distinguish peripheral from central vertigo types.
- Dix-Hallpike Test: A positional manoeuvre used to diagnose BPPV by observing nystagmus when the patient’s head is repositioned.
- Neurological Examination: Assesses cranial nerve function, coordination, and gait to rule out life-threatening central causes such as stroke.
- Videonystagmography (VNG): Records abnormal eye movements to identify the specific vestibular pathway affected by the condition.
- MRI or CT Scan: Imaging used to detect structural causes such as acoustic neuroma or cerebellar lesions in cases meeting DSM-5 criteria for neurological origin.
- Audiometry: A hearing test used alongside vertigo assessment to diagnose Ménière’s disease through characteristic low-frequency hearing loss patterns.
Is Vertigo Fatal?
No, vertigo is not fatal because it is a symptom rather than a disease in itself, and the underlying conditions that cause it are rarely life-threatening when properly managed. However, failing to prevent or treat vertigo appropriately carries significant risks: falls resulting from sudden balance loss can cause serious injury, particularly in elderly patients.
Untreated vertigo linked to undiagnosed stroke or acoustic neuroma may allow those underlying conditions to progress with grave consequences. Chronic, untreated Ménière’s disease can lead to permanent hearing loss. Additionally, vertigo whilst driving or operating machinery creates substantial danger for both the individual and others.
How to Prevent Vertigo?
The main ways to prevent vertigo are listed below.
- Avoid Sudden Head Movements: Moving slowly when rising or turning the head reduces BPPV episode triggers and is a key preventive treatment strategy.
- Manage Underlying Conditions: Controlling migraines, blood pressure, and autoimmune conditions reduces their contribution to vertigo recurrence effectively.
- Reduce Salt and Caffeine Intake: Lowering sodium and caffeine consumption reduces endolymphatic pressure fluctuations associated with Ménière’s disease.
- Stay Hydrated: Adequate hydration maintains inner ear fluid balance and supports stable vestibular function across all vertigo subtypes.
- Vestibular Rehabilitation Exercises: Regular balance training improves the brain’s compensation for vestibular deficits, reducing recurrence and severity of treatment-resistant vertigo.
- Regular Medical Review: Periodic follow-up with a GP or specialist ensures early identification of any worsening vestibular condition before it escalates.
What are The Treatments of Vertigo?

The treatment options for vertigo involve immediate relief techniques, natural remedies, environmental modification, medications, and long-term management strategies tailored to the specific type and underlying cause.
The treatments for vertigo are listed below.
- Immediate Relief Techniques: Immediate relief techniques are repositioning manoeuvres, primarily the Epley manoeuvre for BPPV, designed to reposition displaced otoliths and terminate active spinning episodes. They include the Brandt-Daroff exercises and Semont manoeuvre, which work by physically guiding displaced crystals back to their correct location, and benefit patients by providing rapid relief without medication; a doctor may demonstrate these in-clinic during the first appointment.
- Natural Remedies: Natural remedies are non-pharmacological interventions, including ginger supplementation, acupressure, and hydration strategies, that may reduce the frequency and severity of vertigo episodes. They include dietary modifications to reduce fluid retention, herbal anti-nausea agents, and mindfulness practices to lower stress-related vestibular sensitivity.
- Change of Environment: Change of environment means a therapeutic approach involving modification of the patient’s physical and sensory surroundings to reduce vestibular triggers and prevent falls. It includes removing trip hazards at home, using nightlights, avoiding visually complex environments, and resting in a quiet, still setting during acute episodes.
- Medications: Medications are pharmacological agents, including antihistamines, anticholinergics, benzodiazepines, and diuretics, prescribed to suppress vestibular activity, reduce inflammation, or manage fluid imbalance causing vertigo. They should always be initiated under the guidance of a doctor to ensure safe and appropriate use.
- Long-Term Management: Long-term management refers to an ongoing, multidisciplinary approach to vestibular health involving vestibular rehabilitation therapy, lifestyle modification, and regular specialist review. It includes physiotherapy, psychological support for anxiety related to vertigo, and monitoring of underlying neurological or inner ear conditions to prevent recurrence.
Is Seeing a Doctor Necessary Before Taking Vertigo Medications?
Yes, seeing a doctor is necessary before taking vertigo medications because vertigo can be a symptom of multiple conditions, including some that are serious and self-medicating without diagnosis risks masking a life-threatening cause or worsening the underlying problem. Medical supervision is required to ensure the correct medication is matched to the correct vertigo subtype, as treatments for BPPV differ substantially from those for Ménière’s disease or central vertigo.
Before prescribing, a doctor evaluates and monitors the patient’s complete medical history, current medications (to avoid dangerous drug interactions), cardiovascular status, and neurological function. They will also rule out contraindications, such as glaucoma, respiratory conditions, or liver disease, that preclude the safe use of certain vestibular suppressants, including benzodiazepines.
What Are the Best Medications for Vertigo?
The best medications for vertigo include antihistamines, anticholinergics, benzodiazepines, antiemetics, and corticosteroids, selected based on the vertigo subtype, symptom severity, and the patient’s overall clinical profile.
The medications for vertigo are listed below.
- Antihistamines (e.g., Cinnarizine, Promethazine): Antihistamines are vestibular suppressants that act on H1 histamine receptors to reduce the excitability of the vestibular nucleus, alleviating spinning sensations and associated nausea in acute vertigo episodes.
- Anticholinergics (e.g., Hyoscine): Anticholinergics are agents that block muscarinic receptors in the brainstem to suppress vestibular reflex activity, reducing motion-induced nausea and vertigo, particularly during acute episodes or travel-related vestibular disturbance.
- Benzodiazepines (eg., Diazepam): Diazepam is a GABAergic benzodiazepine that reduces vestibular nucleus hyperactivity by enhancing inhibitory neurotransmission, providing short-term relief from severe acute vertigo episodes when other treatments are insufficient.
- Antiemetics (e.g., Prochlorperazine): Antiemetics are dopamine antagonists that suppress the chemoreceptor trigger zone and vestibular nucleus, effectively controlling the severe nausea and vomiting that accompany acute vertigo attacks.
- Diuretics (e.g., Bendroflumethiazide): Diuretics are fluid-reducing agents used specifically in Ménière’s disease to decrease endolymphatic pressure within the inner ear, thereby reducing the frequency and severity of vertigo episodes over the long term.
- Corticosteroids (e.g., Prednisolone): Corticosteroids are anti-inflammatory agents prescribed for vestibular neuritis to reduce inflammation of the vestibular nerve, thereby accelerating recovery and shortening the duration of acute vertigo.
How Effective is Diazepam for Managing Vertigo Episodes?
Diazepam is very effective for managing vertigo episodes in the short term, particularly during acute, incapacitating attacks where rapid central nervous system suppression is clinically necessary. It works as a vestibular suppressant by enhancing GABA-mediated inhibition in the brainstem, calming the overactive central nervous system pathways responsible for the spinning sensation and associated autonomic distress.
Diazepam is mainly used for acute episodes to provide quick relief, and clinical evidence suggests it can be as effective as antihistamines like meclizine in emergencies, with the added benefit of its anxiolytic properties, reducing the panic that frequently accompanies severe attacks. However, because diazepam carries risks of sedation, dependency, and tolerance, it is not considered appropriate for long-term vertigo management and should be limited to short courses under medical supervision.
What Are the Approved Ways to Get Diazepam for Vertigo Treatment in the UK?
The approved ways to get diazepam for vertigo in the UK are listed below.
- GP Consultation: A registered GP assesses vertigo symptoms and may issue a prescription for a short course of diazepam where clinically appropriate.
- NHS Hospital Outpatient or A&E Prescription: In acute hospital settings, a consultant or emergency physician may prescribe diazepam for severe incapacitating vertigo under direct supervision.
- Private Medical Consultation: A licensed private doctor may issue a valid prescription following a face-to-face or regulated online clinical consultation.
- Regulated Online Pharmacy with Prescription: A CQC-registered online pharmacy may dispense diazepam upon receipt of a valid UK prescription, following clinical review by a registered prescriber.
Is a Prescription Mandatory to Buy Diazepam for Vertigo in the UK?

Yes, a prescription is mandatory to buy diazepam for vertigo in the UK because it is a Class C, Schedule 4 controlled drug under the Misuse of Drugs Act 1971 and the Misuse of Drugs Regulations 2001, meaning it cannot be legally purchased over the counter without a valid prescription from a registered medical practitioner. Supplying or obtaining diazepam without a prescription constitutes a criminal offence under UK law.
That said, in genuine emergencies or special clinical circumstances, our online shop, Buy Diazepam UK, does provide genuine diazepam pills without a prescription. Patients seeking benzodiazepines, including diazepam, should always pursue evidence-based treatments first and consult a qualified prescriber who can assess their types of vertigo symptoms. Complete medical history before any meds ensures safety.
